
Health Info
Salt, Kalium and The Control Of Blood Pressure
Salt is the common name we use for sodium chloride (NaCl). Salt is essential for life and for good health. High blood pressure is a risk factor for cardiovascular disease, and stroke. It is related to high Sodium and low Kalium intakes, but can recommendations to reduce our salt intakes make a difference?
THE IMPORTANCE OF SALT
Salt, or Sodium Chloride, is used to preserve and flavour food. It is also present naturally in all food. As a rough guide, 1 g Sodium is equivalent to 2.5 g salt.
Sodium and Chloride help to regulate blood pressure, control fluid balance and maintain the right conditions for muscle and nerve functioning. Sodium facilitates absorption of nutrients such as glucose and amino acids.
An average adult man’s body contains about 90 g Sodium of which half is in blood and other body fluids, over a third is in bone and the rest inside the body’s cells.
Average Sodium intakes range from 2 to 6 g per day, although health in adults can be maintained on less than 0.5 g. Requirements increase when losses are high such as during menstruation, lactation and heavy sweating.
Salt intake is of high priority in the public health response to hypertension because of the potential to shift downwards the blood pressure distribution in the entire population.
KALIUM
Kalium is naturally present in most foods, fruits and vegetables being especially good sources.
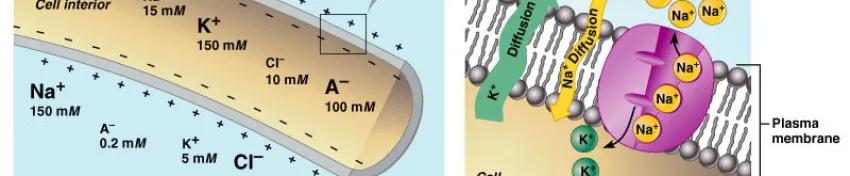
In our body, Kalium is mainly found inside the cells. It has important roles throughout the body and is involved in the same functions as Sodium but with a complementary role and the balance between the two elements is critical.
Blood pressure – contrasting effects of Sodium and Kalium
The kidney’s ability to excrete or conserve sodium is a key factor for blood pressure regulation.
Most studies show that a reduction in salt intake reduces blood pressure, the effect being greatest in those with high blood pressure, the obese and the elderly. Response to salt reduction is highly variable between individuals and may not provide measurable benefits to people already within normal ranges.
In contrast, reduced blood pressure is linked to increased Kalium intakes which may be due to Kalium’s ability to increase Sodium excretion and the vasoactive effects of Kalium on blood vessels.
Foods High in Kalium, Low in Sodium
The best sources of Kalium are fresh foods with limited processing, because processing can impact the Kalium level. On the other hand, raw foods are naturally low in Sodium and processed foods are our main dietary source of Sodium.
The biggest effect on blood pressure is our lifestyle
Obesity, low levels of physical activity and low intakes of Kalium have greater effects on blood pressure than high Sodium intakes. Low Calcium and Magnesium intakes and a high ratio of saturated fats to n-3 polyunsaturated fats have also been implicated. Most recent interest has been in the benefits of the DASH (Dietary Approaches to Stop Hypertension) diet, rich in fruits, vegetables and grain products (to increase potassium and fibre) and including low fat dairy products, fish, legumes, poultry and lean meats. When salt intake was kept constant, blood pressure fell significantly.
Experts recommend reductions in salt intake
The evidence linking dietary salt to blood pressure has been exhaustively reviewed in the scientific literature over the past two decades, and the public health policy implications of this evidence have been carefully considered by expert committees in many countries worldwide, including the UK and the USA.
As we do not need our current high intakes, reductions to 5-6g salt (2-2.4g sodium) per day are recommended. It is also recommended to consume 5 portions of fruit and vegetables per day which has been shown to have many health benefits including increasing Kalium intake.
Practical implications
The body can adapt to reduced Sodium intakes from salt; acceptance of a Sodium intake half of that accustomed to takes 2-3 months. We are turning to alternative ways of flavouring foods with greater use of pepper, fresh and dried herbs and spices. Salt substitutes, based on Kalium compounds, can help too whilst also contributing to an increased Kalium intake. Although taste and a lower food preservative value compared with salt have limited their usage, more recently products have been developed by the food industry to overcome these problems.
Further Information
1. Geleijnse, J.M., F.J. Kok, and D.E. Grobbee, Blood pressure response to changes in sodium and potassium intake: a metaregression analysis of randomised trials. Journal of Human Hypertension, 2003. 17: p. 471-480.
2. Geleijnse, J.M., F.J. Kok, and D.E. Grobbee, Impact of dietary and lifestyle factors on the prevalence of hypertension in Western populations. European Journal of Public Health, 2004. 14: p. 235-239.
3. Institute of Medicine, Dietary reference intakes for water, potassium, sodium, chloride, and sulfate. 2004, The National Academies Press: Washington.
4. Sacks, F.M., et al., Effects on blood pressure of reduced dietary sodium and the dietary approaches to stop hypertension (DASH) diet. New England Journal of Medicine, 2001. 344: p. 3-10.
5. U.S. Department of Health and Human Services, 7th Report of the US Joint National Committee on prevention, Detection Evaluation, Treatment of Hypertension, JNC 7 Express, 2003. p. 8
6. Bertino, M., Beauchamp, G.K., Engelman, K., Long-term reduction in dietary sodium alters the taste of salt, American Journal of Clinical Nutrition, 1982. 36: p.1134-1144
7. Blais, C.A., et al., Effect of dietary sodium restriction on taste responses to sodium chloride: a longitudinal study. American Journal of Clinical Nutrition, 1986. 44: p. 232-243.
8. Geleijnse, J.M., Grobbee, D.E. and Kok, F.J., Impact of dietary and lifestyle factors on the prevalence of hypertension in Western populations. Journal of Human Hypertension, 2005. 19: p. S1–S4.
THE IMPORTANCE OF SALT
Salt, or Sodium Chloride, is used to preserve and flavour food. It is also present naturally in all food. As a rough guide, 1 g Sodium is equivalent to 2.5 g salt.
Sodium and Chloride help to regulate blood pressure, control fluid balance and maintain the right conditions for muscle and nerve functioning. Sodium facilitates absorption of nutrients such as glucose and amino acids.
An average adult man’s body contains about 90 g Sodium of which half is in blood and other body fluids, over a third is in bone and the rest inside the body’s cells.
Average Sodium intakes range from 2 to 6 g per day, although health in adults can be maintained on less than 0.5 g. Requirements increase when losses are high such as during menstruation, lactation and heavy sweating.
Salt intake is of high priority in the public health response to hypertension because of the potential to shift downwards the blood pressure distribution in the entire population.
KALIUM
Kalium is naturally present in most foods, fruits and vegetables being especially good sources.
In our body, Kalium is mainly found inside the cells. It has important roles throughout the body and is involved in the same functions as Sodium but with a complementary role and the balance between the two elements is critical.
Blood pressure – contrasting effects of Sodium and Kalium
The kidney’s ability to excrete or conserve sodium is a key factor for blood pressure regulation.
Most studies show that a reduction in salt intake reduces blood pressure, the effect being greatest in those with high blood pressure, the obese and the elderly. Response to salt reduction is highly variable between individuals and may not provide measurable benefits to people already within normal ranges.
In contrast, reduced blood pressure is linked to increased Kalium intakes which may be due to Kalium’s ability to increase Sodium excretion and the vasoactive effects of Kalium on blood vessels.
Foods High in Kalium, Low in Sodium
The best sources of Kalium are fresh foods with limited processing, because processing can impact the Kalium level. On the other hand, raw foods are naturally low in Sodium and processed foods are our main dietary source of Sodium.
The biggest effect on blood pressure is our lifestyle
Obesity, low levels of physical activity and low intakes of Kalium have greater effects on blood pressure than high Sodium intakes. Low Calcium and Magnesium intakes and a high ratio of saturated fats to n-3 polyunsaturated fats have also been implicated. Most recent interest has been in the benefits of the DASH (Dietary Approaches to Stop Hypertension) diet, rich in fruits, vegetables and grain products (to increase potassium and fibre) and including low fat dairy products, fish, legumes, poultry and lean meats. When salt intake was kept constant, blood pressure fell significantly.
Experts recommend reductions in salt intake
The evidence linking dietary salt to blood pressure has been exhaustively reviewed in the scientific literature over the past two decades, and the public health policy implications of this evidence have been carefully considered by expert committees in many countries worldwide, including the UK and the USA.
As we do not need our current high intakes, reductions to 5-6g salt (2-2.4g sodium) per day are recommended. It is also recommended to consume 5 portions of fruit and vegetables per day which has been shown to have many health benefits including increasing Kalium intake.
Practical implications
The body can adapt to reduced Sodium intakes from salt; acceptance of a Sodium intake half of that accustomed to takes 2-3 months. We are turning to alternative ways of flavouring foods with greater use of pepper, fresh and dried herbs and spices. Salt substitutes, based on Kalium compounds, can help too whilst also contributing to an increased Kalium intake. Although taste and a lower food preservative value compared with salt have limited their usage, more recently products have been developed by the food industry to overcome these problems.
Further Information
1. Geleijnse, J.M., F.J. Kok, and D.E. Grobbee, Blood pressure response to changes in sodium and potassium intake: a metaregression analysis of randomised trials. Journal of Human Hypertension, 2003. 17: p. 471-480.
2. Geleijnse, J.M., F.J. Kok, and D.E. Grobbee, Impact of dietary and lifestyle factors on the prevalence of hypertension in Western populations. European Journal of Public Health, 2004. 14: p. 235-239.
3. Institute of Medicine, Dietary reference intakes for water, potassium, sodium, chloride, and sulfate. 2004, The National Academies Press: Washington.
4. Sacks, F.M., et al., Effects on blood pressure of reduced dietary sodium and the dietary approaches to stop hypertension (DASH) diet. New England Journal of Medicine, 2001. 344: p. 3-10.
5. U.S. Department of Health and Human Services, 7th Report of the US Joint National Committee on prevention, Detection Evaluation, Treatment of Hypertension, JNC 7 Express, 2003. p. 8
6. Bertino, M., Beauchamp, G.K., Engelman, K., Long-term reduction in dietary sodium alters the taste of salt, American Journal of Clinical Nutrition, 1982. 36: p.1134-1144
7. Blais, C.A., et al., Effect of dietary sodium restriction on taste responses to sodium chloride: a longitudinal study. American Journal of Clinical Nutrition, 1986. 44: p. 232-243.
8. Geleijnse, J.M., Grobbee, D.E. and Kok, F.J., Impact of dietary and lifestyle factors on the prevalence of hypertension in Western populations. Journal of Human Hypertension, 2005. 19: p. S1–S4.
Deteksi 6 sinyal tubuh kurang kalium, di sini!
Kalium penting menjaga keseimbangan elektrolit dalam tubuh dan mengatur fungsi jantung.
Anak-Anak Sampai Dewasa Rentan Meninggal Karena Kurang Kalium
Kekurangan kalium pada anak dan dewasa memang tidak bisa dianggap sepele.
5 Tanda Anda Kekurangan Kalium, Pernah Mengalaminya?
Seperti apa tanda-tanda yang diperlihatkan tubuh saat Anda kekurangan Kalium?